
For centuries, man has been drinking. A certain percentage of the population seems to like the effect produced by alcohol a little too much and suffer from alcoholism. Are they born that way, or have they developed a craving that they can’t control? If so, why can’t they control it? Could the problem be nature or nurture? Is it a biological, psychological or physiological problem?
Alcoholism: Moral Failing or Disease?
Many who live with a problem drinker believe that the problem is a matter of willpower or a lack of moral character. Why can’t he or she just stop? Don’t they see what it’s doing to them and their loved ones? There is a common misconception that the alcoholic has a choice once the first drink has been consumed, but in fact, most alcoholics don’t.
The medical community states that alcoholism is a disease not a choice, but many families, acquaintances, co-workers, friends, and clergy think of alcoholism as a moral failing. They think if he or she would just turn their problem over to God, or pull themselves up by their bootstraps, they could beat this alcohol thing. Stop it, just stop it.
Alcoholism is a Disease and Not a Moral Failing
I have been on both sides of this argument as I suffered from the slings and arrows of my family, friends and business associates. It is my assertion that alcoholism is a disease and not a moral failing. I will offer information on both sides of the argument, which I believe will help the reader understand why this is considered a disease, and why morality has nothing to do with it.
“In the Crucial Phase, the alcoholic has work and money problems, experiences tremors, starts to drink in the morning and experiences persistent remorse. Then there is a third phase, the “Chronic Phase”. In this phase, the alcoholic is obsessed with drinking, drinks with inferiors, and admits complete defeat.”
The History of Alcoholism
This paper will present a historical perspective on the problem and where the misinformation, misconceptions, and confusion might have originated. “The word “alcohol” is derived from the Arabic al kohl. Nineteenth-century temperance advocates tried to prove that the word “alcohol” is derived from the Arabic al Ghul, meaning ghost or evil spirit” (Kinney 2).
The problem with drinking came to be known as dipsomania. According to The Merriam-Webster Dictionary, dipsomania is “an uncontrollable craving for alcoholic liquors.” This term later morphed into alcoholism in the middle 19th century.
“Throughout history, alcohol has been the most popular psychoactive substance” (Inaba 1.5).
For centuries, ancient societies used and abused alcohol and other substances, for their pleasure. There is evidence that ancient civilizations used alcohol naturally fermented from fruit over 50,000 years ago, but most evidence points to the sustained use of alcohol over 10,000 years ago. As civilization grew and became more sophisticated, the need for comfort through alcohol and other mind-altering substance also grew. “Many ancient cultures considered alcohol, particularly wine, a gift from the Gods” (Inaba 1.6).
Temperance in China
As the cultures and mankind developed, so did the production of various liquors. Just as today, some of the earliest people did not know when enough was enough. “One of the earliest attempts at temperance occurred in China around 2200 B.C. when legendary Emperor Yu levied a tax on wine to curtail consumption” (Inaba 1.6). Later in China, as most everywhere else penalties for public intoxication could be drastic for lower class people while the upper class was allowed more leniency (Inaba).
No one culture, religion, or ethnic group has been able to escape the drinking problem. It was true in the Neolithic period, and it is true today. While most people use alcohol responsibly, there are those who can’t, once they consume one drink, a thousand drinks not enough, and as you will see has nothing to do with lack of willpower.
Research on Alcoholism
Over the years sustained research studies into alcoholism have been conducted in the United States and elsewhere. Why did alcohol affect some more than others, and why when one would start drinking, have no ability to stop?
In 1941 E. M Jellinek, along with Carl Bowman, presented their research on alcoholism treatment. They concluded that there were twenty-four classifications of alcoholism, covering four types of alcoholics (Inaba).
Jellinek, who came to be known as the father of alcoholic studies, was a biochemist that loved working with statistics. He made alcohol studies his life’s work. He continued his research and in 1952, published a study charting signs and symptoms associated with alcohol addiction. “The work was based on a survey of more than 2,000 members of AA. Although differences certainly existed among individuals, to him the similarities were striking” (Kinney 87).
The Jellinek Curve+
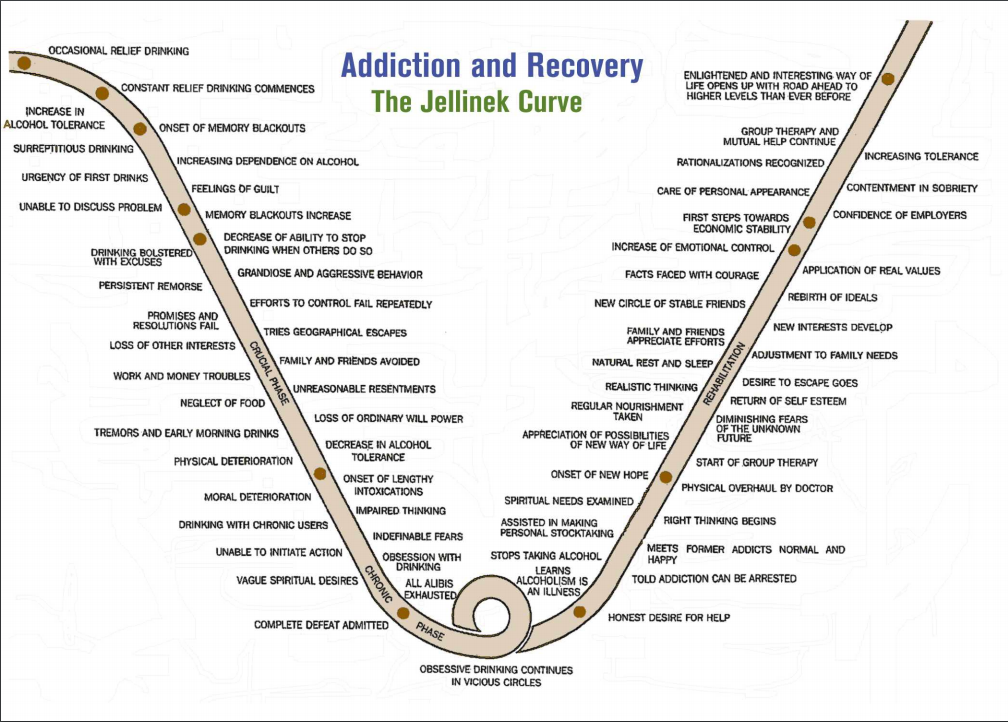
As part of that study, he published what has come to be known as “The Jellinek Curve.” The curve charted his findings, in part explaining certain phases of the problem drinker.
The first phase being the “Prodromal Phase.” It starts with occasional relief drinking and soon advances to blackout drinking and an inability to talk about the problem, coupled with an increased dependence on alcohol.
The second phase is described as the “Crucial Phase.” In the Crucial Phase, the alcoholic has work and money problems, experiences tremors, starts to drink in the morning and experiences persistent remorse.
Then there is a third phase, the “Chronic Phase.” In this phase, the alcoholic is obsessed with drinking, drinks with inferiors, and admits complete defeat.
The 5 Types of Alcoholism
In 1960, eight years later, Jellinek wrote a book; The Disease Concept of Alcoholism, which contends that alcoholism, is a disease. In the book, Jellinek states that there are five types of alcoholism: alpha, beta, delta, gamma, and epsilon.
- Alpha state is presenting a purely psychological picture, there is no loss of control or inability to stop.
- Beta state represents physical problems, such as cirrhosis, or alcoholic hepatitis.
- Gamma state is typically recognized as a change intolerance leading to withdrawal symptoms and loss of control.
- Delta state is similar to the Gamma state in that there is physiological and physical dependence but no loss of control.
- Epsilon state remains a periodic state. Meaning that the dependent alcoholic is not a daily drinker but a periodic drinker, otherwise known as a binge drinker.
Jellinek’s work went a long way in creating a modern concept of alcohol dependency, and the idea of alcoholism as a disease. The medical and psychiatric communities have also come to see alcoholism as a disease. “In 1956, the American Medical Association (AMA) stated alcoholism was a disease, as it met the five criteria needed to be considered a disease: pattern of symptoms, chronic, progression, subject to relapse, and treatability” (AlcoholismFacts).
Also Read: 7 Signs of Alcoholism That Your Drinking May Be Getting Out Of Hand
Alcoholism Defined
The American Psychiatric Association, which publishes the DSM-V, has alcohol-related disorders listed in the category of Substance-Related and Addictive Disorders. The DSM-IV describes alcohol use disorder this way; “The problematic pattern of alcohol use leading to clinically significant impairment or distress, as to manifest by at least two of the following, occurring within a twelve month period.”
It then goes on to list eleven such illustrations. The National Institute on Alcohol Abuse and Alcoholism states: “Alcohol use disorders are medical conditions that doctors can diagnose when a patient’s drinking causes distress or harm.”
The World Health Organization prefers to recognize the problem as Alcohol Dependence Syndrome, as in the DSM-IV. In 1993, the American Society of Addiction Medicine, a professional association of physician’s specializing in substance abuse issued the following statement:
“Alcoholism is a primary, chronic disease with genetic, psychological and environmental factors influencing its development and manifestations. The disease is often progressive and fatal. It is characterized by continuous or sporadic impaired control over drinking, preoccupation with the drug alcohol, use of alcohol despite adverse consequences, and distortions in thinking, most notably denial…” (Kinney 81)
ASAM goes out of its way to explain the fact that they think of alcoholism as a disease. They state simply that they think of disease as an “involuntary disability.” (Kinney 81)
This is one side of the argument, but there are those that don’t buy the idea of alcoholism as a disease, and they are quite insistent about it.
The Flaws in Alcoholism Research
There are many scholars and scientists who do not necessarily agree with Jellinek’s theory or AMA’s assertion. They believe the disease model is a flawed experiment, and if anything, it should be thought of in a social context instead of a medical one.They believe that if the Jellinek’s Disease Concept is accepted as true, then it is the research, in this assumption, that is flawed.
Dr. Herbert Fingarette, a professor at the University of California and a consultant on alcoholism and addiction to the World Health Organization, disputes this idea in his book, Heavy Drinking, The Myth of Alcoholism As A Disease. Fingarette says “There is no adequate empirical substantiation for the basic tenets of the classic disease concept of alcoholism” (Fingarette 3). He goes on to say “proper scientific differences of opinion do remain about the relevance of the term disease to some forms of chronic heavy drinking” (Fingarette 22).
Dr. Fingarette goes on to assert that because Jellinek’s original work was based on a questionnaire sent out to AA members with only 158 respondents out of 2,000 questioners sent, the science is without question suspect. Fingarette asserts that of the 158 respondents, 60 were held back because it appeared that they had pooled their answers together. Women were excluded from the data because their answers differed so greatly from the men. (Fingarette)
Alcoholism as a Behavior Issue
Dr. David J. Hanson is a teacher in the Sociology Department at the University of New York, in Potsdam. He states, “The debate over whether alcoholism is a disease or simply a behavioral problem has continued for over 200 hundred years and doesn’t appear likely to end soon” (Is Alcoholism A Disease). Dr. Hanson studied Jellinek’s research based on the AA members questioner and asserted that even Jellinek later recognized the inadequacies of his hypothesis(Is Alcoholism A Disease). As the reader can see, there is considerable disagreement as to the disease concept of alcoholism.
Psychiatrist Dr. Morris Chafert, the first director of the NIAAA, was a long-term advocate of the disease concept. He stated; “Having experienced the extent of my prejudices and my ignorance of the issue, I was bound and determined to turn the country around and to treat alcoholics as ill human beings who needed treatment, not as bad people who should be ignored and neglected” (Grimes).
Dr. Chafert was originally not sympathetic to the alcoholic or their plight. Over the course of his career, he came to see the desperation in the alcoholic and realized that this was not so much a moral problem as it was a medical one. On the other hand, we have those who view the alcohol question regarding a moral question. As most people see it, there are two ways of looking at the morality question, immoral or amoral.
“The immoralists view the alcoholic as not having morals. They also use words such as “sinful” or “moral weaklings” when describing alcoholics. At the other extreme, amoralists divorce morality from alcoholism citing the disease concept as evidence. The amoralist tells a patient/client: “You’re not a bad person trying to get good, you’re a sick person trying to get well!” (Stole)
Alcoholics Struggle with Their Morality
Despite what people think, many alcoholics constantly endure a deep and constant internal struggle on morality. The day after a spree can be a terrible time for alcoholics. The feelings of guilt, shame, and powerlessness can be overwhelming. Many alcoholics have these feelings because their actions are not in line with their morals, and therefore, they feel helpless. “The fact is that most alcoholics, for reasons yet obscure, have lost the power of choice in drink” (Wilson 24).
Alcoholics show surprise when after many a promise, they drink again. They seem to have no mental defense against the first drink. Their morality seems their actions, slipping further and further down the line as Jellinek illustrates in his curve. This behavior will not change until According to Bill Wilson, (Co-founder of AA) they experience a “psychic change.” The immoralists are unable or unwilling to accept this moral struggle. The moralist only helps the problem drinker by offering therapy and a sympathetic ear.
The Physiology of Alcoholism
“Without question, the brain is the organ that is most sensitive to the acute effects of alcohol.” (Kinney 61) Pleasure Unwoven is a documentary film that looks very closely at how the brain responds to addiction. Dr. Kevin Mc Cauley is the host of the film and guides us through the concept that states the midbrain and the frontal cortex play a huge part in addiction.
Research shows that in using alcohol, parts of this brain activate and in effect create a pleasure center. This area is known as the reward system of the brain. It includes several elements, such as the ventral tegmental area, the nucleus accumbus septic, the lateral hypothalamus, and the prefrontal cortex (Inaba 2.17). Seeking the reward area in the brain leaves the addict defenseless.
In determining whether an alcoholic is suffering from a disease, we need to restate what the disease model is. The disease model that physicians use, today looks something like this. The disease model states, you have an organ, the organ gets a defect, and as a result, you get symptoms. The Dr. goes about working on the defect, and hopefully, the organ soon shows no more symptoms. The advent of this concept in medicine over the last 100 years has doubled life expectancy.
“In the last twenty years, there has been an explosion of understanding about the brain and addiction. Today neuroscientists do know the parts of the brain involved in addiction. They know the nature of the defect, and that defect and that organ show that the behaviors of addicts are in fact symptoms of the disease.” (Mc Cauley 16:15)
How the Brain Reacts to Alcohol
According to Mc Cauley, there are two areas of the brain that play a major role, the midbrain, and the frontal cortex. The frontal cortex is where we evaluate the world around us. This is where choice conceives(Mc Cauley). The frontal cortex is where we attach, emotions, thinking, moral, social, and spiritual choices.
We believe that addiction starts in the midbrain. “The midbrain does not think; it does not make choices or understand consequences. Instead, it handles the next fifteen seconds. It gets us from moment to moment, alive” (Mc Cauley 22:00).
The midbrain tells us when to eat, when to fight and when to procreate. These instincts are critical to survival. The midbrain makes these events pleasurable. Typically, the frontal cortex keeps the midbrain in check, but with addiction, that control fails, and the midbrain takes more control in guiding behavior than the frontal cortex (Mc Cauley). “In addiction, something goes wrong at a level of brain processing long before morals, personality or choice” (Mc Cauley 23:00).
In addiction, the drug hijacks the survival mechanism of the midbrain, thereby replacing the midbrains natural order. The drug now becomes the primary force, and alters the midbrain’s ability to function properly. The drug now equates to survival. Once this happens, we have crossed into addiction (Mc Cauley). As far as the midbrain is concerned alcohol is no longer alcohol, it represents how to get through the next 15 seconds alive.
Pleasure Processed by the MidBrain
The brain’s pleasure sense lies deep into our midbrain. As mentioned before the midbrain does not think, it acts and handles the next 15 seconds. In addiction, the pleasure sense shows itself compromised or broken. “Addiction is a defect in the brain’s ability to perceive, process and act upon pleasurable experiences” (Mc Cauley 28:00). When the brain creates a pleasurable experience, it brings many layers of processing together. When thinking of a pleasurable experience we remember smells, places, and emotions that lie dormant for years, but at the onset of pleasurable thought, the memories come flooding back. The brain brings them together into one memory. “In addiction, something goes wrong at every level of brain processing” (Mc Cauley 31:10).
Alcoholism and Genetics
Genetics has a lot to do with who will become alcohol dependent and who won’t: “Genes can create differences in how people respond to drugs” (Mc Cauley 34:25). A study in San Diego found that genes play a huge role in how people respond to alcohol. Some people have a genetic predisposition for alcoholism, but genetics alone is not enough. There are also some environmental concerns. The environment can change the way genes act and perform. Take, for instance, an adult that is a recovering alcoholic. That person passes on his biological genetic makeup to his or her offspring, but they also pass along their sobriety. He passes all the work that went into that recovery along to the children.
Dopamine
The release of the chemical dopamine by the neurons in the midbrain is the earliest response from a pleasurable experience. “Dopamine tells the brain when a reward is better than expected. The dopamine acts as a learning signal, to help identify, prioritize and then anticipate if an experience was better or worse than expected” (Mc Cauley). Drugs cause a surge of dopamine, far more than the brain can handle.
The surge of dopamine tricks the brain into thinking that drugs are much better than expected. Each time an alcoholic uses alcohol, the release of dopamine tells the brain that it was far better than expected; therefore, it is necessary for survival. This sets up the moral question very well. Why would someone continue to use alcohol even thought each time they use it something terrible happens. It is because, after persistent use, they have altered their brain chemistry and now drinking is not merely a pleasurable experience, but the pleasure center demands it. Neurologically speaking, individuals have no choice. The midbrain is signaling that this substance is necessary for survival.
Glutamate
When the brain finds something good for survival, it needs to remember it. This is where glutamate comes into play. Glutamate is the chemical that helps with memory function. “It is the chemical which allows for drug memory and drug seeking” (Mc Cauley 45:10). The dopamine neurons send their rewards up from the ventral tegmental area and the nucleus accumbus toward the frontal cortex, while the glutamate neurons send their rewards down from the frontal cortex back down to the midbrain.
The introduction of drugs or alcohol into the brain destroys the delicate neurological balance and wipes out natural processes. With time drug pathways become stronger and stronger and natural pathways weaker and weaker. “This is no longer a natural memory it becomes a hyper memory, and perhaps permanent” (Mc Cauley 47:00). In alcoholism, the normal top-down control from the frontal cortex down to the midbrain fails. As this happens, the addict has no mental or moral defense against the first drink, drug, pill or fix. They are biologically incapable of staying away from or making an informed decision. “We are unable, at certain times, to bring into our consciousness with sufficient force the memory of the suffering and humiliation of even a week or a month ago. We are without defense against the first drink” (Wilson 24).
Alcohol Does Not Discriminate
The disease of Alcoholism is an equal opportunity destroyer. The disease doesn’t discriminate based on gender, age, race, ethnicity, education, employment status, geographic region, marital status, or religion. As described in this paper, a moral failing or a lack of character does not cause alcoholism. If triggered, it is a biological certainty. The psychoactive agents involved in alcohol, and the brain’s reaction to it, end up hijacking the old brain. The brain then believes that the consumption of alcohol is more important than life itself.
Jellinek was onto something when he started his research about alcohol and its addictive powers. His methods show flaws as originally presented, but the research opened the door to continued studies and a firmer understanding of what addiction looks like. With the data present today, Dr. Fingarette may not be so critical of the disease concept. He addresses most, if not all, of the objections he presents in his book. It appears that there exists empirical evidence that alcohol addiction is real, and the disease concept roots itself in fact.

